
What does a doctor do to know the cause and best treatment options for my ED? The Diagnosis of Erectile Dysfunction involves history taking, physical examination, a blood sample and imaging. In most cases, the Diagnosis of ED can be reached in 1-3 days.



Causes of ED can wither be psychological ( psychogenic ED ) or disease-related ( organic ED ), and is mostly treatable.
Contents
1-History Taking for the Diagnosis of ED
a-Morning erection / nocturnal erection:
Diagnosis of ED involves asking about nocturnal erections. Normally, one experiences a rigid erection when he wakes up every now and then. This is “Morning erection” or “nocturnal erection”.
Presence of normal morning erection is a sign that impotence is psychogenic rather than organic.
To explain this, during sleep, one is relieved of psychological stress that prevents erection in day time, but is not present to prevent erection that normally occurs at sleep. On the contrary, if there is an organic cause to impotence, erection will occur neither in day time nor at sleep.
Inquiring about morning erection for the Diagnosis of Erectile Dysfunction may not always meet an accurate answer. The method for objective evaluation of the nocturnal erection: the rigiscan (see later).
b-Inquiring about causes and predisposing factors for impotence:
Some data can help the Diagnosis of Erectile Dysfunction: inquiring about the cause of impotence such as the presence of psychological stress, symptoms suggestive of hypertension (headache, bleeding nose, drowsiness), symptoms suggestive of diabetes (frequent urination, frequent thirst and hunger, family history of diabetes)..etc
c-The international Index of Erectile Function IIEF
IIEF is a questionnaire of five questions about erectile function. The gentleman choses one of five answers, each with a score. The total score for all questions indicates whether or not one has ED and how severe it is. You can take the IIEF questionnaire and receive a preliminary Diagnosis of Erectile Dysfunction on our website. Click here.
2-Clinical Examination for the Diagnosis of Erectile Dysfunction:
For the diagnosis of ED , physical examination can point to signs of hormonal imbalance, abnormal development of the genitalia and local diseases of the penis such as fibrosis..etc.
3- Investigations for the diagnosis of ED
In case there is high suspicion of organic impotence or there is failure of response to treatment, investigations are necessary:
Blood Sugar Analysis: It is one of the most important lab analyses for the diagnosis of erectile dysfunction and is considered routine in many practices. It points out to the presence of diabetes which is one of the most common causes of impotence.
A blood sample is taken after 8 hours of fasting (no eating or drinking sugary fluids), then another sample is taken 2 hours after eating.
Glucose (sugar) concentration in tissues is particularly important and should be normalized before surgery in cases of severe impotence. It is again measured by a blood sample. and is called HBA1c or Glycated Hemoglobin.
Hormone Analysis: This is particularly important for the diagnosis of ED in older patients where there is natural decline in testosterone levels, or in those with signs of hormone imbalance such as lack of body hair (though not a conclusive sign).
A blood sample is taken in day time, early morning (9-11AM) to take the biological clock and the normal hormone level fluctuations into consideration. Testosterone and prolactin are measured. Testosterone is measured in terms of free testosterone and total testosterone.
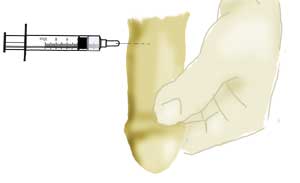
Intra-corporal Injection (ICI):
This is injection of PGE1 or other medications that induce erection directly into the penis. These chemicals are either vasodilators or muscle relaxants.
In normal subjects, ICI should result in a rigid erection that starts in 5 minutes time and lasts for at least 30 minutes.
In subjects with organic impotence, erection may not occur at all, or may be less than the minimum encountered in normal subjects.
For the diagnosis of erectile dysfunction, erection is graded on a scale from E0 to E5, where E5 is the normal rigid erection that persists for 30 minutes.
If response to ICI is less than optimum, further investigations are required to specify the diseased part: arteries? veins?..etc. The next investigation is Penile Duplex.
It has to be noted that both normal subjects and subjects with organic impotence due to nerve disease preventing neuronal transmission may respond in an exaggerated pattern to ICI with a rigid erection that lasts for hours.
ICI
Penile Duplex / Penile Ultrasonography for the diagnosis of erectile dysfunction:
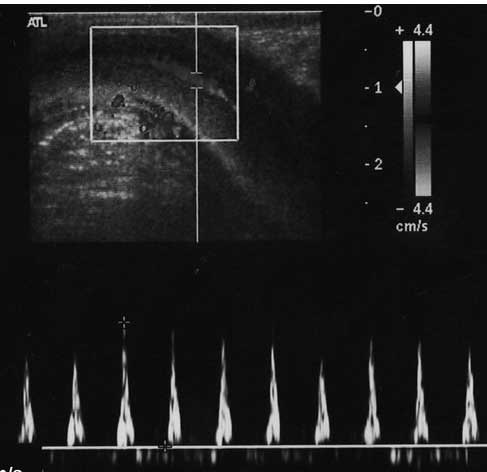
Ultrasonography can inspect the interior of the penis for fibrosis,arterial occlusion orvenous leak. In order to evaluate arteries and veins, erection is induced by intra-corporal injection (see before).
Normal arterial flow should be more than 25cm/second, while normal venous flow should be less than 5cm/second. Normally there should be no fibrosis or calcification in the penis. If there is, penile duplex can determine their position, extent, and relation to vital structures of the penis.
Cavernosometry:
If duplex points to the possibility of venous leak, this has to be confirmed by cavernometry, where erection is induced by intra-corporal injection (see before), and the pressure inside the penis is measured by a needle connected to a sphygmomanometer.
Cavernosography for the diagnosis of erectile dysfunction:
If cavernosometry confirms the presence of venous leak, the exact position and distribution of the leaking veins is determined by cavernosography. A dye is injected in the penis after induction of erection using intra-corporal injection (see before). Normally, the dye should be trapped in the penis together with blood. If there is a leak, the dye seeps out of the penis through veins. These veins can be imaged and localized by roentgenograms.
Measuring Nocturnal Erection / Morning Erection: RIGISCAN for the diagnosis of erectile dysfunction:
As described before, the occurrence of normal morning erection or nocturnal erection is indicative of the cause of impotence being psychological. However, simple questioning about morning erection may not always give accurate results.
Rigiscan is a device that can help with the diagnosis of erectile dysfunction by measuring erection that occurs at sleep, and can determine how many times it has occurred, for how long, and how large was the diameter of the penis at erection, and thereby the circumferential rigidity (side to side rigidity).
Rigiscan is composed of a portable unit that is attached to the thigh, from which emerge two wires, each attached to a sensitive coil that is worn around a penis. The device is used by the patient for 3 consecutive nights, to be worn at bed time. The coils record changes in the penis and transmit them to the recording unit around the thigh, from which data is downloaded and plotted as a graph at the end of the examination.
Unfortunately, circumferential rigidity measured by rigiscan is of minor importance in erection . Axial rigidity is the most important. The latter is rigidity along the length of the penis that prevents it from bucking if pressure is applied to the glans towards the abdomen, just like normal intercourse. Thus, rigiscan is not conclusive for the diagnosis of ED and is therefore not a routine investigation.